HULC treats many conditions affecting the hand, wrist and elbow. Should your condition or injury not be listed below, please call us to discuss how we treat it.
Conditions
Arthritis
Arthritis is a common condition affecting many joints of the body. It can be caused by damage to the joints through wear and tear as we age, previous injuries and various autoimmune diseases.
The base of the thumb is a common joint for arthritis to affect. Treatment options depend on the joints involved and the severity and duration of symptoms. Non-operative treatment options include splinting and exercises. There are many different surgical options available for trapeziometacarpal joint (basal thumb) arthritis. While many surgeons remove the entire trapezium, we have found that partial resection of the trapezium produces the best functional outcome with resolution of pain. This procedure is done through 2 small ‘keyhole’ (arthroscopic) portals.

Biceps and Triceps Rupture
This is usually an injury which will need surgical repair. If you think you have ruptured your triceps or biceps tendon and are having difficulty straightening or bending your elbow you should see your GP and ask for a specialist hand surgeon referral.
The therapists at the Hand and Upper Limb Centre can help with your rehabilitation post surgery. Usually your recovery will involve initially protecting the arm in a sling or splint and then starting some gentle movements. Once tendon strength has returned you may be able to commence some strengthening and stretching exercises.


Carpal Tunnel Syndrome
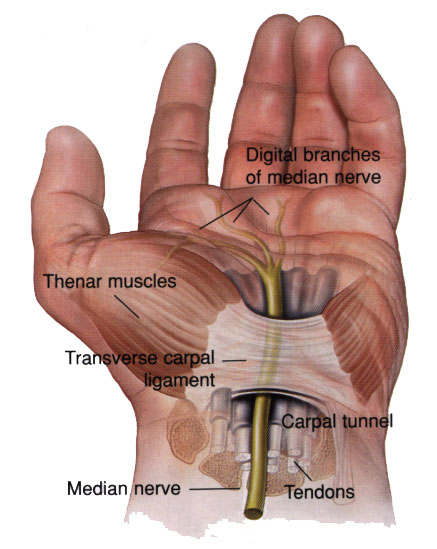
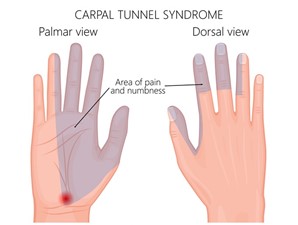
Carpal tunnel syndrome is the most common nerve compression that affects the hand and wrist. It’s caused by pressure on the median nerve, usually from swelling. The median nerve runs the length of the arm, passing through a passage in the wrist called the carpal tunnel and ending in the hand. The median nerve controls the movement and feeling of the thumb and all fingers except your small finger.
Symptoms of carpal tunnel syndrome usually include pins and needles, numbness and pain in the thumb, index and middle finger. If you have carpal tunnel syndrome and don’t get it treated, symptoms can last a long time, get worse, and can even go away and return. Carpal tunnel is easier to treat if diagnosed earlier.
We commonly treat carpal tunnel syndrome and beneficial treatment can include splinting to rest the nerve, home exercise programs and modification of daily activities.
Various nerves can also be compressed at other areas in the upper limb including the elbow, shoulder and neck. Therapists at HULC are specialists in assessing and treating a variety of nerve conditions. Your therapist is trained in assessing whether a surgical review is warranted depending on the history and severity of your symptoms.


De Quervain’s Tenosynovitis
De Quervain’s tenosynovitis has been described as an inflammation of the tendons that straighten and pull the thumb back. Latest research indicates that it is more associated with tendon degeneration and microtrauma of the tendons.
Repetitive movement, excessive and accumulative strain of the thumb and wrist is commonly the cause of De Quervain’s. It can also be the result of an acute injury.
Typical symptoms include pain with thumb/wrist movement, swelling over the affected area and difficulty with functional use. Recent or expectant mothers and individuals who have job requirements of a particularly repetitive nature are most at risk of experiencing De Quervain’s tenosynovitis. For this reason, De Quervain’s tenosynovitis, may also be called ‘mum thumb’ or ‘washer women’s wrist’.
In mild to moderate cases of De Quervain’s tenosynovitis, hand therapy can be very effective. Therapy usually involves a combination of splinting, soft tissue treatment, activity modification and a graded strengthening program.

Distal Radius Fractures
The radius is one of two bones that make up the forearm. A distal radius fracture means a fracture of the radius bone has occurred near the end of the bone, close to the wrist. A fracture to a distal radius may also be called a broken wrist or Colles Fracture.
Distal radius fractures are one of the most common injuries treated at HULC. In fact, the radius is the most commonly broken bone in the arm.
Distal radius fractures often occur as a result of a fall on an outstretched hand. Fractures are normally diagnosed with an X-ray. Symptoms can include pain, swelling, bruising and an inability to use the affected hand.
Many fractures may be treated in a custom made thermoplastic splint which protects the bone whilst it is healing. However, some fractures require surgery to ensure correct alignment. This may include an internal fixation i.e. plate and screws or a manipulation under anesthetic.


Dupuytren’s Contracture
Dupuytren’s Fibrosis is a genetic condition where your fingers are pulled into your palm by thickening of the tissue under the skin. It is more common in men, people of northern European descent and onset is generally delayed until the 4th and 5th decade of life.
A referral to a surgeon is required for treatment. Consequently, HULC has set up a pioneering ‘Dupuytren’s Clinic’, the first clinic of its kind, together with eminent hand surgeon Mr Jeff Ecker.
Our highly trained Dupuytren’s Fibrosis hand therapists run this clinic to measure the hands every 6–12 months to detect progression or extension of the condition and intervene before there is major contracture. This way, people can have simple minimal intervention to control the disorder and delay or avoid major complex surgery.
Our therapists work closely with your surgeon to oversee and monitor your condition. We assist in post-operative management of this condition, including wound care, splinting, scar management and regaining movement.
HULC is active in researching the best surgical and post-operative treatment for this condition.


Elbow Dislocations
The majority of elbow dislocations can be treated with closed reduction (putting the joint back into the correct position) and protected range of motion in a hinge splint. Your therapist will be able to guide you with activity restrictions and start you on an early motion program to minimise post-injury stiffness.
A word of warning – Injuries to the elbow joint can be difficult to treat. The joint is very complex and prone to becoming very stiff. Recent research has shown that the sooner movement is commenced post injury, the better the outcome for the patient.


Elbow Fractures
There are two bones in your forearm, the radius and ulna. They hinge with the humerus bone (this is the long bone located between the elbow and the shoulder) in your arm to form your elbow joint. Any of these bones may be fractured (broken) in a fall or injury to your elbow. Common parts of these bones which fracture at the elbow include:
- The distal humerus – Distal means further from the centre of the body. This forms the top part of the joint that helps us bend and straighten our arm.
- The radial head – (this is top part of the radius) is made entirely out of cartilage. It helps us turn our hand to face upwards and down wards (supination/pronation)
- Olecranon – this is the very top part of the ulna bone. It forms the bottom part of the joint which helps us straighten and bend our elbow.
Fractures to the elbow joint can be difficult to treat. The joint is very complex and prone to becoming very stiff. Usually a splint or sling is used to align and stabilise the fracture for bone healing. If your fracture is stable and does not need surgery it is advised to start gently moving your elbow immediately. Recent research has shown that the sooner movement is commenced post injury the better the outcome for the patient. Your therapist will help you determine when it is best to start moving your elbow and also advise you on whether you should consider seeking a specialist opinion.
Finger Dislocations
Finger dislocations are one of the most common injuries we treat, particularly in sports people. The most common joint to injure is the Proximal Interphalangeal joint (the middle joint of your finger).
Joints are surrounded by soft tissue to allow them to move with stability. When a joint is dislocated some of these structures are invariably damaged. A custom-made splint is recommended to protect the soft tissues as they heal, whilst hand therapy will prevent the joint from stiffening.

Fractures
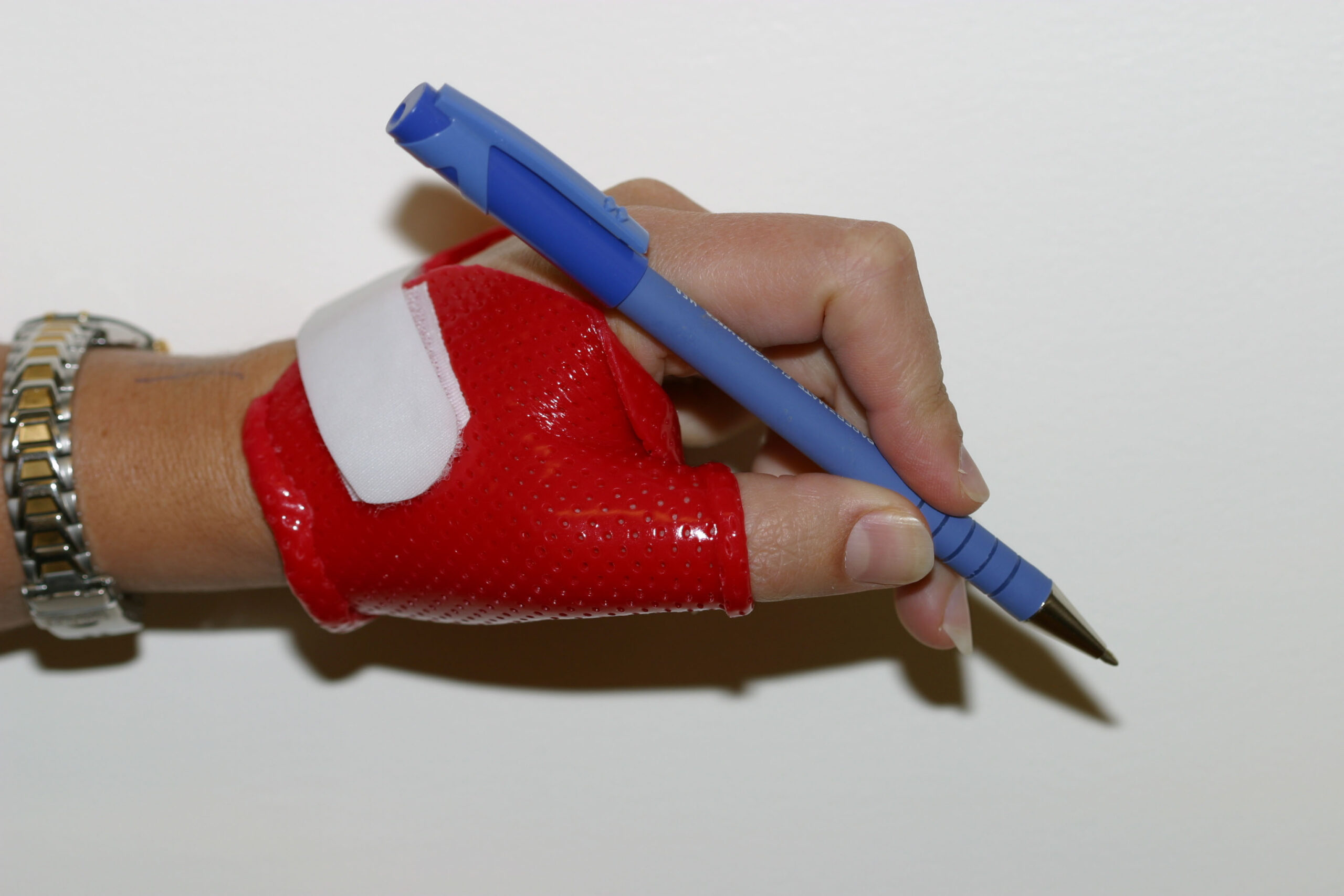
The words fracture and breaks are interchangeable when talking about bones. Simple fractures that are in alignment can be treated by immobilising the finger, hand or wrist. At HULC we are specialists in making custom-made, lightweight thermoplastic splints, also known as an orthosis, to support the fracture whilst it heals. These splints are made to measure at your first appointment and can be modified if your hand/wrist changes shape, due to factors such as a reduction in swelling. Another bonus is these splints can get wet! For complex breaks that require surgery to fix and align the bones, a splint can be made post-operatively.
Hand therapy is vital in the case of any hand or wrist fracture to optimise movement and function post injury.

Keinbock’s Disease
Keinbock’s disease is not something which can be treated alone with hand therapy. If you suspect you have Keinbock’s disease you should see your GP and ask for a specialist hand surgeon referral. Your GP may also suggest an X-ray to assess the health of your lunate (a small moonshaped carpal bone).
Ligament Injury to the Wrist
The wrist is a very complex joint. With many ligaments connecting the eight small carpal bones, the metacarpals and bones of the forearm. The most common wrist ligament injuries occur to the TFCC and Scapholunate Dissociation.
Your therapist has a complex understanding of the wrist joint and will be able to assess which ligament group is most likely injured. Sometimes an MRI or functional view X-rays may be requested for your GP to order.
Lymphoedema
Lymphoedema is abnormal swelling that generally occurs in one of the arms or legs. Sometimes both arms or both legs swell. Lymphoedema is most commonly caused by the removal of, or damage to lymph nodes as a result of cancer treatment. This causes a blockage in the lymphatic system (which is part of your immune system) preventing the lymph fluid from draining well, thus leading to fluid build-up and swelling.
Lymphoedema can be managed with early diagnosis and diligent care of your affected limb, including self-management techniques and the fitting of compression garments.
All HULC therapists are trained in the prescription of custom made Jobst and Alvarex compression garments for the upper limb. Occupational Therapist Emma Simpson also provides a management service for patients with simple upper limb Lymphoedema in our Bunbury and Busselton clinics. Ellen Gulin provides this service in our metro clinics. Patients in the community who need ongoing management for their lymphoedema can be seen at HULC, who will then liaise with their specialist service for formal reviews.
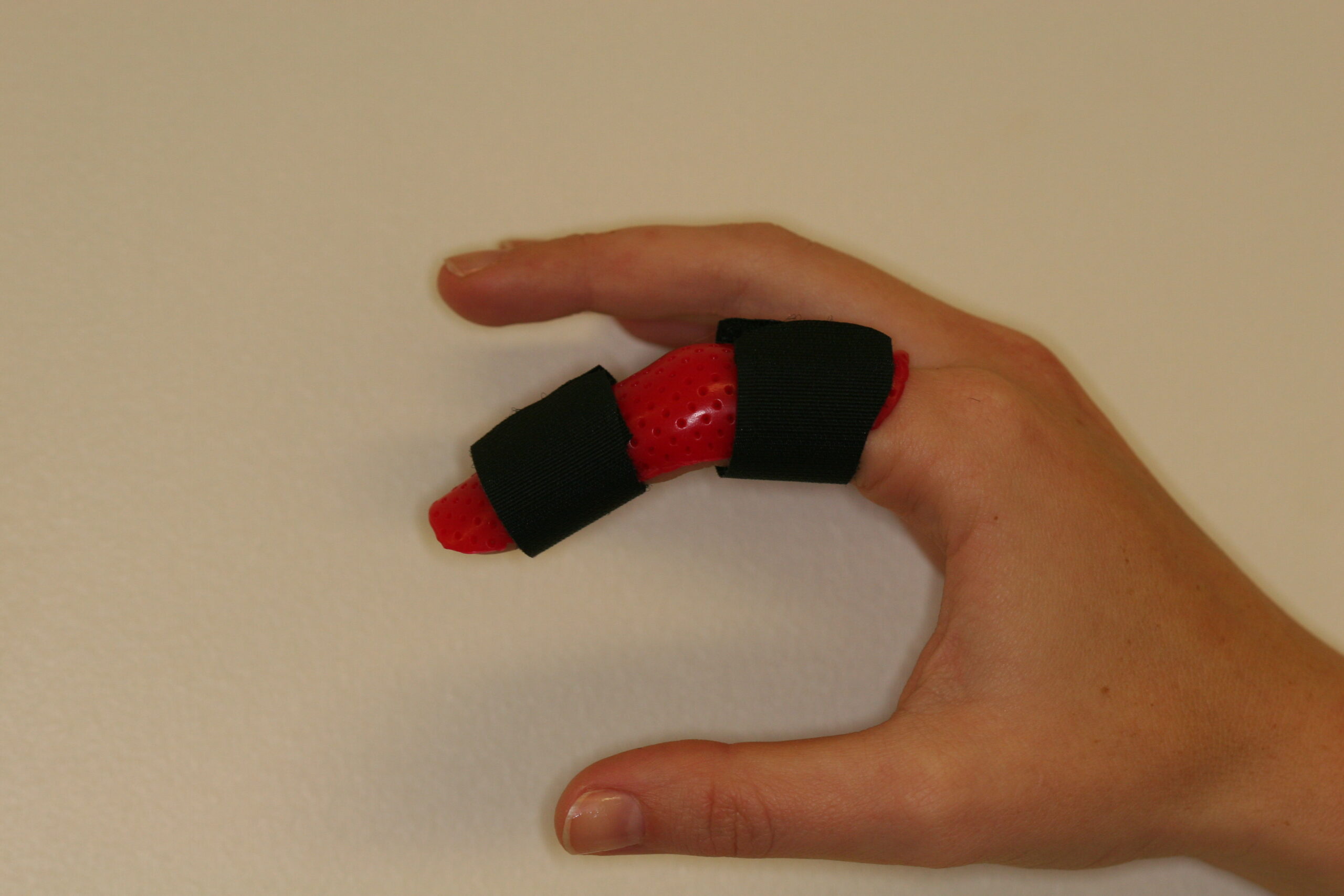
Mallet Finger
Mallet finger is a very common condition seen in our practice. It is commonly caused by a ball hitting the end of the finger, however there are various other causes. This results in damage to the tendon that straightens the end joint of the finger. The finger will usually appear bent and is often painful and swollen.
Immediate splinting is the best treatment to correct the deformity and assist in healing. An X-ray is required to see if this is associated with a fracture of the finger.
Nerve Compression
Various nerves can be compressed in the upper limb at various locations, including the wrist, elbow, shoulder and neck.
This includes:- Carpal Tunnel Syndrome
- Guyons Canal Compression
- Cubital Tunnel Syndrome
- Radial Tunnel Syndrome
The Occupational Therapists at HULC are trained in assessing and treating a variety of nerve conditions. Your therapist will be able to identify the affected nerve and ascertain the best treatment for you. This may involve use of a splint (usually at night), some special nerve exercises and help with ergonomic modification.
Occasionally, people have severe nerve compression. In this case a specialist review or nerve conduction study may be warranted. Your therapist will be able to guide you if this is the case.
Paediatric (Children’s) Hand Injuries
Our team frequently works with children and their caregivers to assess and treat broken bones or other types of upper limb trauma.
Given children are still growing, it is essential these injuries are assessed and treated in a timely manner to prevent long term complications. Fractures that displace or compress the growing part of the bone can be particularly serious.
Our team are able to fit a custom water-proof thermoplastic splint or fibreglass cast for acute fractures/dislocations or help out with a play based hand exercise program. They will also be able to discuss with you if a specialist paediatric hand surgeon opinion is warranted.
Please note, if your child has received care from the Perth Children’s Hospital for an upper limb injury we require a referral to remove the cast and place them in a thermoplastic splint. A recent X-ray is also helpful and allows your therapist to appropriately assess the injury.
Scaphoid Fractures
The Scaphoid is one of the small carpal bones in the wrist. Scaphoid fractures are most commonly caused by a fall on an outstretched hand.
Symptoms generally include pain at the base of the thumb which is worse with use of the hand, tenderness and swelling. X-ray is required to confirm diagnosis; however sometimes scaphoid fractures can go unnoticed and even an x-ray may not reveal a fracture. Careful assessment and referral on for more investigations is sometimes needed if a scaphoid fracture is suspected.
The scaphoid is a slow healing bone due to it’s poor blood supply. Some scaphoid fractures can be treated in a custom made thermoplastic splint which protects the bone whilst it is healing. Some fractures require surgery to ensure healing and correct alignment.

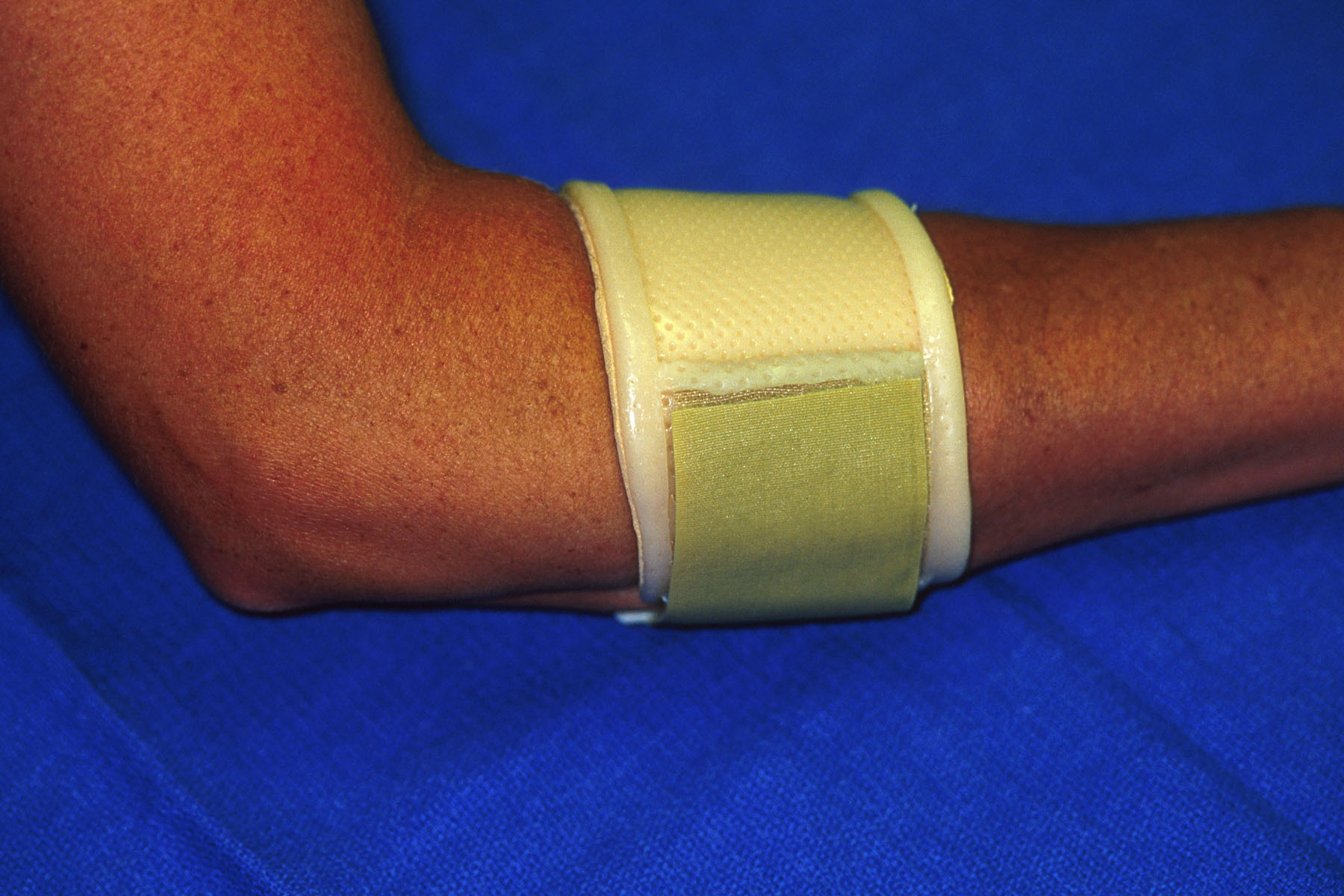
Tennis Elbow / Golfers Elbow
Lateral epicondylitis (more commonly known as tennis elbow) is a degenerative condition of the tendons that attach onto the bony prominence (epicondyle) on the outside (lateral side) of the elbow. The tendons are attached to the muscles that lift (extend) the wrist and hand.
Individuals who develop this condition are usually involved in work or recreational activities that require repetitive and vigorous use of the forearm muscles.
Symptoms may include aching pain on the outside of the elbow or a sharp pain that radiates from the elbow down the forearm. Symptoms are often aggravated by lifting and repetitive forceful gripping.
There are numerous non-operative therapy options which can be used to treat lateral epicondylitis. These include ice, heat, splinting, bracing, massage, ergonomic modification and strengthening programs. Often treatment will involve more than one technique. Your therapist will be able to assess your tennis elbow and let you know which treatments are likely to work best for you.
Medial Epicondylitis (more commonly known as golfers elbow) is much less common than tennis elbow and affects the tendons on the inside of the elbow. The tendons are attached to muscles that drop (flex) the wrist and hand. It is treated in a similar way to tennis elbow.
Triangular Fibrocartilage Complex (TFCC)
As the name indicates, this is a complex collection of structures that work together to stabilise and support the wrist and facilitate placement of the hand for functional activities.
Traumatic and chronic disruption to the TFCC is a common cause of ulnar-sided wrist pain and is often associated with decreased grip strength and impaired function.The main functions of the TFCC are:
- To stabilise the ‘distal radio-ulna joint’, the joint allows you to rotate your forearm.
- To absorb shock from any forces going through your hand.
How does this injury occur?
- The TFCC is often injured with forced rotation of the forearm. This can happen in a fall, when holding heavy objects or using power tools etc.
- It can also be a chronic ‘wear and tear’ injury – for example if you have a heavy repetitive job, or if your bony anatomy puts extra stress on the ligament.
When an injury occurs, it means the ligament has been disrupted. This might be a tear in the ligament, the ligament may have stretched, become too thin, or pulled away from the bone.
Some injuries are treated with surgery to repair the ligament, others may rest in a splint or special wrist band, and other may be treated with exercises to strengthen the wrist. Your therapist will be able to guide you as to which treatment is most suitable.
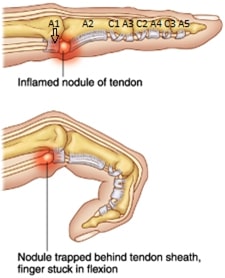
Trigger Finger
Trigger finger can occur when one or more of the tendons that bend your finger thicken or enlarge. It then has trouble moving through a pulley. This can result in locking of the finger in a bent position and pain when trying to straighten the finger. Splinting can be an effective treatment for this condition as it allows the inflammation to settle and the tendon to reduce in size.

Wrist Pain
The wrist is a very complex joint. Pain can be caused by a number of things, including inflammation, ligament strains/ tears, overuse injuries, arthritis, hypermobility, old fractures, nerve compression and weakness.
Our therapists are widely experienced in treating the many causes of wrist pain and use a number of different treatment tools and techniques to help relieve pain and maximize mobility.